More on KentOnline
More on KentOnline
A harrowing report reveals 45 baby deaths could have been prevented in east Kent with proper care.
The results of a large-scale investigation into maternity failings at East Kent Hospitals NHS University Trust, dubbed the Kirkup Review, have been released today.

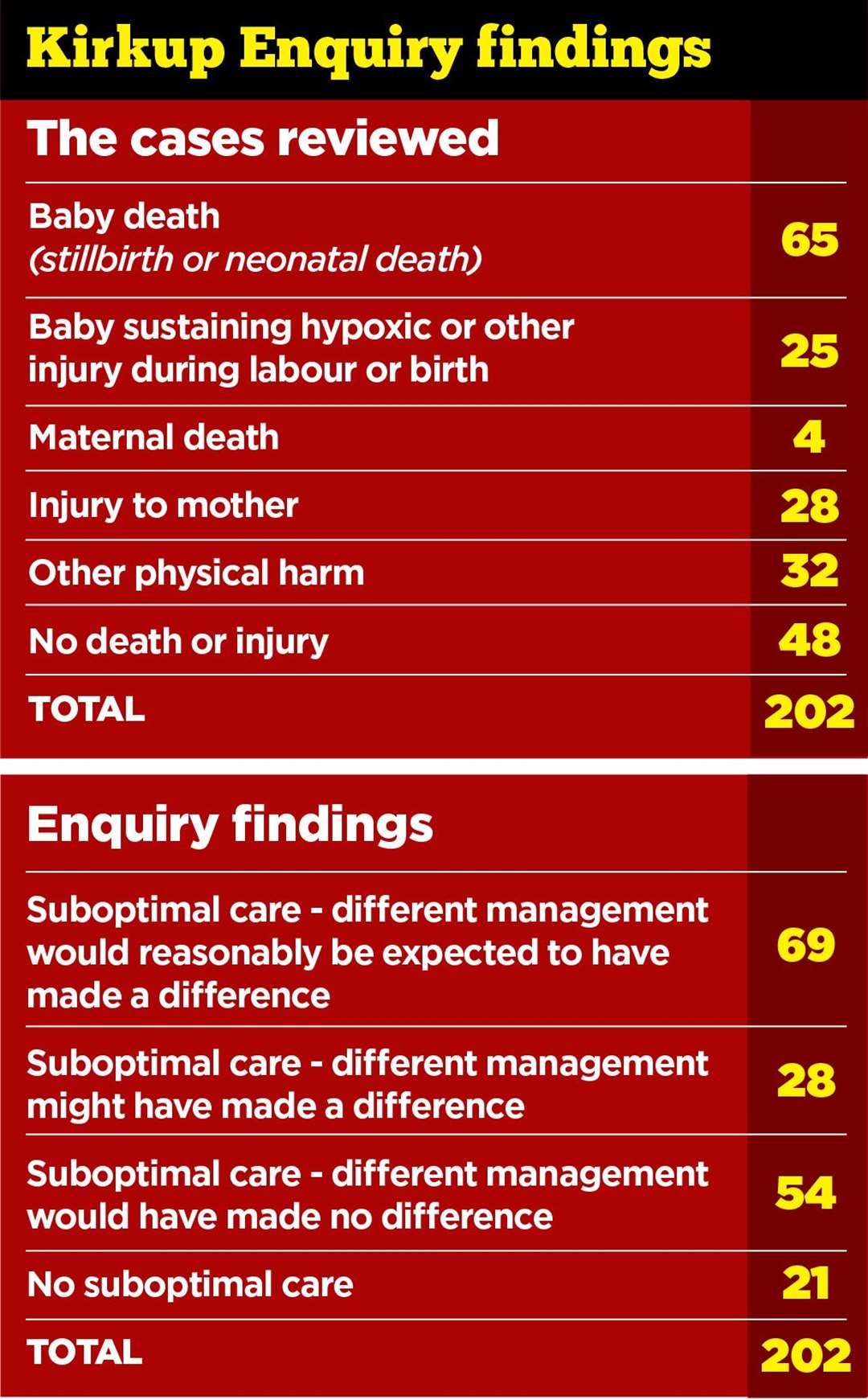
In total, more than 200 cases dating back to 2009 have been looked at by an expert panel chaired by Dr Bill Kirkup, who also led the investigation into mother and baby deaths in Morecambe Bay in 2015.
Figures among the literature show that if care been given to nationally recognised standards, the outcome could have been different in 97 of the total 202 cases reviewed –a total of 48%.
The data also shows 45 of 65 baby deaths could have been prevented if appropriate care had been given.
In relation to cases of injury to babies, the panel found the outcome could have been different in 12 of the 17 cases of brain damage.
When it came to maternal injuries and deaths, it was found the outcome could have been different in 23 of 32 such cases.
But in his report, Dr Kirkup says he has "no doubt" there are more cases of failings that the panel hadn't even investigated.
The report also highlighted “clear and repeated” failures of professionalism from staff at the hospitals.
It is noted that staff were disrespectful to women and disparaging to colleagues in front of them.
Others sought to deflect responsibility, some even blaming the mothers themselves for their own misfortune.
There were also failures in teamworking, compassion and listening, the report reveals.

Included in the document was some of the reported comments told to patients and their partners.
One husband recalled a midwife saying of his wife: “She’s making the wrong call here, and it’s going to be your wife’s fault when it all goes wrong."
Another woman reported the comments of a consultant about a colleague: "[They’re] all over the place because [they’ve] just come back from a cruise."
Another woman was told: “Under no circumstances can you leave this room. If you do, you are putting your unborn child at risk … on your head be it."
The report states: "Time after time, we heard that staff not only failed to show compassion, they also denied responsibility for what had happened, or even that anything untoward had occurred.
"Similarly, we have found instances where the mother was blamed for what had happened.
“Where things went wrong, clinical staff, managers and senior managers often failed to communicate openly with families about what had happened.
"The instinct was to minimise what had happened and to provide false reassurance, rather than to acknowledge errors openly and to learn from them."
The trust failed to successfully address known issues with midwifery and obstetric staff, the investigation found.
In addition, it found it easier to attribute causes of specific cases of wrongdoing to individual clinical error, usually on the behalf of more junior staff.
Furthermore, Dr Kirkup states the panel has "not been able to detect any discernible improvement in outcomes or suboptimal care, as evidenced by the cases assessed over the period from 2009 to 2020".
He adds: "We have no doubt that these numbers are minimum estimates of the frequency of harm over the period.
"We made no attempt to review other records or to contact families who did not volunteer themselves.
"It was our judgement that we had enough evidence based on the existing 202 cases to identify the problems and their causes, and we did not wish to delay publication of our findings."
Speaking at a press conference today, Dr Kirkup said there was a "great deal of pain and anger" from the families over the report.
He said drastic changes were needed: "This cannot go on. We cannot go on treating failures as one offs. I do not want to be in this position again."
Four key action areas have been identified in the report. These are:

From those areas, the report made a number of key recommendations, including the establishment of a Task Force "for mandatory national use" to help find "significant trends and outliers" in welfare reports.
It also suggested that the government reconsider bringing forward a bill placing a duty on public bodies "not to deny, deflect and conceal information from families and other bodies".
Finally, it recommended that "the trust accept the reality of these findings; acknowledge in full the unnecessary harm that has been caused; and embark on a restorative process addressing the problems identified".
Speaking following the release of the report, Kelli Rudolph, whose baby Celandine Rudolph died in 2016, said: "It was only over time and also in the lead-up to today's report that we've discovered the scale of the problem at the trust.
"And so we realised that we're part of a large pattern and that was very disturbing.
"It's what we expected and many others have expected it too - but it doesn't make it any less harrowing.
"But there's some relief in knowing the truth is out there. The facts have been laid out clearly."
East Kent Hospitals University NHS Foundation Trust runs five hospitals in total, with its main maternity services at the Queen Elizabeth The Queen Mother Hospital (QEQM) in Margate and the William Harvey Hospital in Ashford.

The trusts's chief executive, Tracey Fletcher, said today: “I want to say sorry and apologise unreservedly for the harm and suffering that has been experienced by the women and babies who were within our care, together with their families, as described in today’s report.
"These families came to us expecting that we would care for them safely, and we failed them.
"We must now learn from and act on this report; for those who have taken part in the investigation, for those who we will care for in the future, and for our local communities. I know that everyone at the Trust is committed to doing that.
"In the last few years we have worked hard to improve our services and have invested to increase the numbers of midwives and doctors, in staff training, and in listening to and acting on feedback from the people who receive our care.

"While we have made progress, we know there is more for us to do and we absolutely accept that. Now that we have received the report, we will read it in full and the Board will use its recommendations to continue to make improvements so that we are providing the safe, high-quality care our patients expect and deserve.
"I want every family – whether they contributed to the investigation or not – to know I am here to listen to them, to learn and to lead our Trust in acting on this report.
"I would like to thank Dr Bill Kirkup and the investigation team for their work.
"Today, our thoughts remain with those who have shared their experiences. We are grateful to them.”
The government is expected to respond today to Dr Kirkup's report, which was commissioned by NHS England in 2020 following growing concerns about quality of care.
Sir Roger Gale, MP for North Thanet said of the findings: “Having been involved in the matter from the time when these concerns and failings first came to light and having been instrumental in instigating the independent inquiry I hope that the parents and families who have suffered will feel that while nothing will never eradicate their losses at the very least Dr Kirkup has fairly and thoroughly exposed on their behalf what has gone wrong in the past and what further measures need to be taken to ensure that no families will in the future ever have to endure such painful and devastating experiences.

“There have been, I believe, serious failings in middle-management that remain to be resolved and there has been a lack of honesty and transparency that has been wholly unacceptable and has exacerbated the suffering of parents. That has to change.”
Dover and Deal MP Natalie Elphicke said: “Today’s report makes such shocking reading.
"These avoidable baby deaths have devastated so many Kent families, including the parents of Tallulah-Rai in Dover.
“Tallulah-Rai should now have been nearly three years old. It’s so tragic that she never even got to take her first breath.
“Families have fought long and hard for improvements so that other parents don’t have to go through the heartbreak and pain they have suffered.
"Today’s landmark report is a testament to the commitment and dedication of each and every one of them.
“It is so important that East Kent Hospitals listen and learn from this report."
Last October, the Care Quality Commission (CQC), which inspects hospitals, again expressed concerns over the trust, which it has repeatedly ranked as “requires improvement”.
It said that during unannounced inspections in July 2021 there were not enough midwifery staff and maternity support workers to keep women and babies safe.

Inspectors said staff were feeling exhausted, stressed and anxious, while some community midwives had taken on additional work in the acute units, which meant they were sometimes working 20-hour days.
In 2020, the Healthcare Safety Investigation Branch (HSIB), which investigates NHS harm, detailed how, despite repeated warnings from its investigators, improvements were not made to maternity care at the trust.
The HSIB began working with East Kent’s maternity units in 2018 and identified “recurrent safety risks” including over how CTG readings were interpreted, baby resuscitation, recognition of deterioration in mothers and babies, and the willingness of staff to escalate their concerns to more senior medics.
From December 2018, the HSIB said it “engaged frequently” with the trust about its concerns but kept seeing the same things happening.
In August 2019, it asked the trust to self-refer to the CQC and regional health bosses.