More on KentOnline
More on KentOnline
Winter is a time of huge demand at Medway Maritime Hospital, which serves 405,000 across the Towns and neighbouring Swale. Reporter Ed McConnell visited those fighting to maintain a high standard of care while contending with chronic bed shortages.
Descriptions of A&E as a "war zone" and like the "Third World" are not at all helpful, says consultant nurse Cliff Evans.
The veteran medic has worked at 19 hospitals during his 30-year career and is held in high esteem at Medway, where he's credited with transforming a failing emergency department, often described as the facility's "front door".
Cliff's a likeable chap, a burly former Army Reserve nurse who is well qualified to criticise such comparisons.
To his credit he does well to mask what must be considerable frustration.
"Our workforce were quite upset about that, a lot of them come from abroad, from places like Iraq and Syria," he said.
"There may be times when you have a long wait, but there’s no connection between that and the Third World or a war zone.
"There are no bombs going off or people turning up in trucks with limbs blown off.
It’s difficult, even as the person who wrote the offending article, to argue with him.
"I agree that it’s far from a perfect comparison but in my defence that’s what people, and many of them, were saying following a tough few days at the hospital.
“Rightly or wrongly people expect a certain level of care and in their opinion that experience fell way short of that,” I contend.
There were tales of people vomiting in waiting rooms and of a frail octogenarian who waited 24 hours to be sent to a ward. The hospital was elevated to the highest level of alert.
People were understandably frustrated, says Cliff: “If you are waiting here for a bed and you have been seen and treated in the Emergency Department, or you didn’t need to be there in the first place, and you can’t go to specialist areas because they’re full, it’s really frustrating.”
But staff were equally put out because through that period the vast majority of patients were assessed within 15 minutes.
When Cliff arrived at the hospital in 2016 his concerns about safety left him unable to sleep.

Three years on he says things have come on leaps and bounds.
He said: “The trust certainly needed to be in special measures.
“We had one of the highest mortality rates in the country.
"We don’t anymore - the last results I saw we were sitting just below the national average.
"You had people waiting two hours for triage; as a result people could die, you cannot have that.”
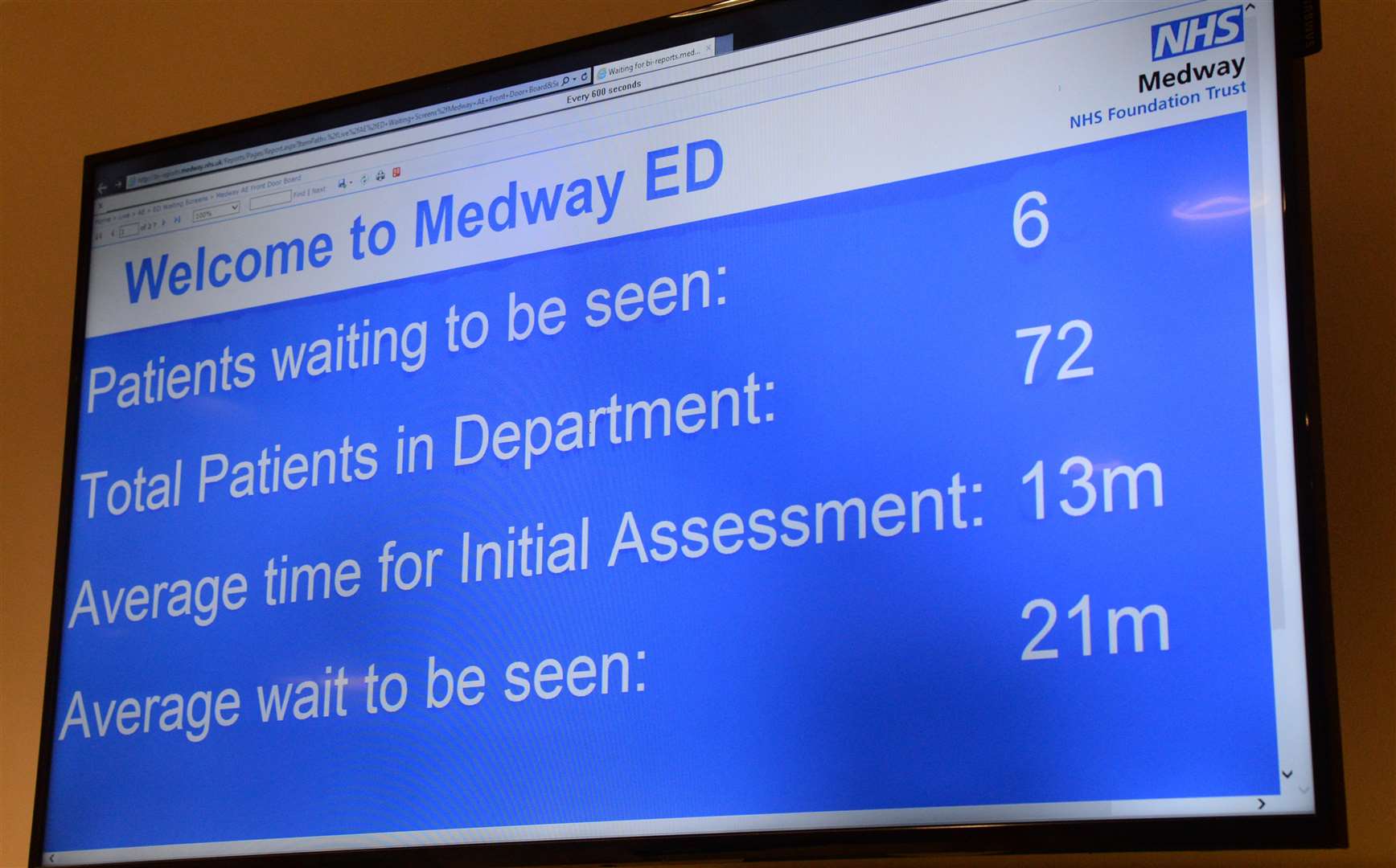
That is why the 15-minute target is so important. It’s not imposed upon the hospital but rather one it’s come up with, and it’s working.

On the Monday before I met Cliff, 441 people presenting at the new £11 million Emergency Department made it the second busiest day ever, but of those only 38% remained there after being assessed by a doctor.
The rest either went home or were sent to MedOCC, the hospital’s in-house GP service.
It is a system that, says Cliff, means emergency cases are being seen faster than ever before, with those coming by ambulance seen as soon as they arrive.
One of those is 64-year-old Southeastern employee Thomas McGilloway, of Eastcourt Lane, Twydall, who is patiently sat in the waiting room.
Suffering from chest pains he phoned 111 and ended up being taken to the hospital by ambulance.
Almost as soon as the brakes were applied the dad-of-six and grandfather-of-12 was receiving a heart scan.
“The staff go out of their way to try and help," he said.
“The wait can be long but the hospital has definitely improved since about five years ago."
Back when Cliff arrived, someone like Thomas may well have still been sat in the back of an ambulance at this point, but now with improved facilities and processes his experience will be vastly different.
One of the final pieces in the jigsaw is how, if need be, to best get Thomas to the next step in his journey through the hospital.
To best understand why there’s no quick fix for what is often termed "bed blocking", a trip from the hospital’s front door to its exit is important.
Here presides head of site flow, Michelle Mackie.
"There may be times when you have a long wait, but there’s no connection between that and the Third World or a war zone" - Cliff Evans
The trained nurse leads a staff meeting every morning and several "huddles" through the day.
Huddles see nurses in charge of different wards make the trip down to a room with more screens than Currys to relay the latest information on patients who are able to leave hospital.
Michelle then marks them as either 'discharge' - everything is in place for them to leave hospital; 'query' - some things aren't; and the self-explanatory 'gone' or 'cancel' - they were previously set to go but due to a deterioration they’re not anymore.
The reasons for lengthy wait times and blockages throughout the hospital become clear when the scale of issues are relayed.
Test waits prove a bit of a problem in terms of getting people out of the door but by far the biggest issues relate to arrangements for when these patients, many of whom are elderly, leave hospital.
Cold weather and icy conditions make respiratory problems and broken bones all the more common and for the frail this time of year is not kind.
The concern is that for this age group, visiting hospital is rarely a straightforward process - once the elderly are in a bed getting them back home, where they’re often best off, isn’t simple.

Due to their vulnerability they can’t just be sent packing once they’re deemed well enough.
Measures have to be in place to ensure they’re safe in the community and when it comes to this, something as apparently minor as moving a bed can cause real problems.
When one elderly man’s at home, he and his wife sleep next to each other in specially-adapted beds, but she’s ill and in order to stop him catching it they need to be separated.
Disassembling the bed and shifting it mere metres to the neighbouring room shouldn’t be difficult, but according to the community healthcare team it’s going to take five to 10 working days, meaning a well man will be left in hospital for up to two weeks by which point he could easily be ill again.
On top of that he’s now a "bed blocker" - a brutal term but one which sadly sums the situation up - and is essentially adding to delays at the other end of the hospital.
It’s not an easy situation to resolve but it’s one chief executive James Devine told me is a priority, with a drive under way to improve communication between the hospital and external agencies.
At the other end of the scale is a man who simply doesn’t want to leave.
This can be common with homeless people or some elderly patients who quite like the company hospital can bring, explains Michelle.
There’s also those who can’t wait to leave and self-discharge.
This is prevalent among the young and if there’s a concern about them the bed has to be kept free until they’ve been tracked down.
The end result of all of this is staff end up playing a huge game of Tetris, fitting patients on to the correct ward for their condition and gender while ensuring only fit people leave and doing their best to make that happen.